
+91 - 9848407907
For a Consultation Call Or
Make An Appointment
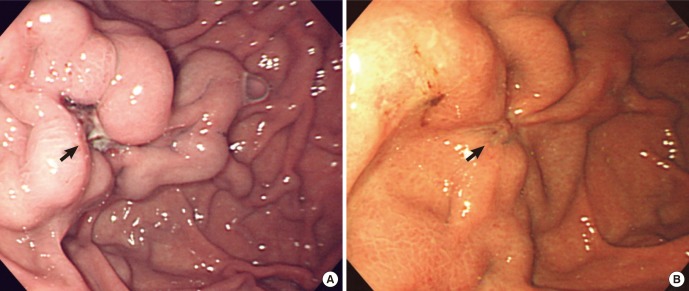
Gastric varices are dilated submucosal veins in the stomach, which can be a life-threatening cause of bleeding in the upper gastrointestinal tract. They are most commonly found in patients with portal hypertension, or elevated pressure in the portal veinsystem, which may be a complication of cirrhosis. Gastric varices may also be found in patients with thrombosis of the splenic vein, into which the short gastric veins which drain the fundus of the stomach flow. The latter may be a complication of acute pancreatitis, pancreatic cancer, or other abdominal tumours, as well as hepatitis C. Gastric varices and associated bleeding are a potential complication of schistosomiasis resulting from portal hypertension.
Patients with bleeding gastric varices can present with bloody vomiting (hematemesis), dark, tarry stools (melena), or rectal bleeding. The bleeding may be brisk, and patients may soon develop shock. Treatment of gastric varices can include injection of the varices with cyanoacrylate glue, or a radiological procedure to decrease the pressure in the portal vein, termed transjugular intrahepatic portosystemic shunt or TIPS. Treatment with intravenous octreotide is also useful to shunt blood flow away from the stomach's circulation. More aggressive treatment including splenectomy (or surgical removal of the spleen) or liver transplantation may be required in some cases.
Initial treatment of bleeding from gastric varices focuses on resuscitation, much as with esophageal varices. This includes administration of fluids, blood products, and antibiotics.
The results from the only two randomized trials comparing band ligation vs cyanoacrylate suggests that endoscopic injection of cyanoacrylate, known as gastric variceal obliteration or GVO is superior to band ligation in preventing rebleeding rates. Cyanoacrylate, a common component in “super glue” is often mixed 1:1 with lipiodol to prevent polymerization in the endoscopy delivery optics, and to show on radiographic imaging. GVO is usually performed in specialized therapeutic endoscopy centers. Complications include sepsis, embolization of glue, and obstruction from polymerization in the lumen of the stomach.
Other techniques for refractory bleeding include:
© All Rights Reserved @ Hardhiks.com 2018.